You can grow beating heart cells and small heart-like tissue structures from stem cells today, and researchers are already testing heart muscle patches in human clinical trials. What you cannot do yet is grow a complete, transplant-ready human heart from scratch. The gap between those two things is enormous, and understanding it is the most useful thing you can take away from this question.
Can You Grow a Heart From Stem Cells? What’s Possible Now

Marcus Whitmore
21 May 2026

What does 'growing a heart' actually mean?
This is where most confusion starts. 'Growing a heart from stem cells' can mean at least three very different things, and the science is at a completely different stage for each one.
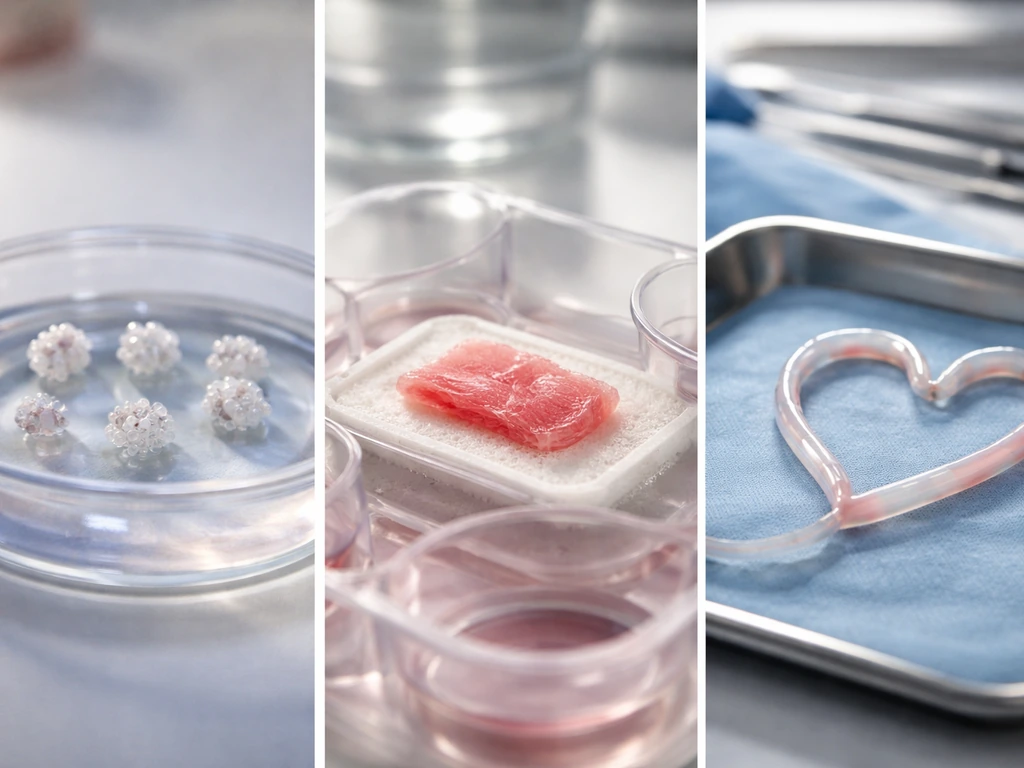
- Cardiac organoids: tiny 3D clusters of heart cells (sometimes called 'cardioids') that beat, show basic chamber-like structures, and model early heart development. These are typically a few millimeters across and are used for research and drug testing, not transplantation.
- Engineered heart tissue patches: larger flat or 3D constructs of aligned cardiomyocytes embedded in a scaffold, designed to be sutured onto a damaged heart to restore some muscle function. These are in early human clinical trials right now.
- A whole functional heart organ: a fully patterned, vascularized, four-chambered organ capable of sustaining a person's circulation after transplantation. This does not exist yet and is not expected within the next decade at minimum.
The 2021 and 2023 literature on human heart organoids is genuinely exciting. Self-assembling hPSC aggregates can form interconnected chamber-like structures with endothelial and epicardial cell markers. But these reproduce early developmental stages, not an adult working heart. Think of it like the difference between a seedling and a mature fruit tree. Same organism, radically different scale and function.
Stem cells and cardiac differentiation: the basics
Stem cells are cells that haven't committed to a final identity yet. The most useful type for heart research are human pluripotent stem cells (hPSCs), which include embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs). iPSCs are especially practical because you can make them from a patient's own skin or blood cells by reprogramming them back to an embryonic-like state. That means the resulting heart cells are genetically matched to the donor, which matters enormously for rejection.
To turn a pluripotent stem cell into a cardiomyocyte (heart muscle cell), you run it through a differentiation protocol that mimics what the embryo does naturally. The process involves carefully timed doses of signaling molecules that push cells down the cardiac lineage. Key pathways involved include Wnt, BMP, FGF, Notch, Sonic hedgehog, and Hippo signaling. The most widely used lab approach today is the 'Wnt-on/Wnt-off' protocol: you activate Wnt signaling early (typically with a molecule called CHIR99021), then inhibit it later (with IWP2 or IWP4). This two-step chemical switch, combined with BMP4, bFGF, and Activin A at specific timepoints, reliably produces a high percentage of cardiomyocytes that start beating spontaneously within a week or two.
The result is real heart muscle cells. They express cardiac-specific proteins like cardiac troponin T (cTnT), they contract rhythmically, and they respond to drugs the way real heart cells do. That's exactly why they're so valuable for disease modeling and drug screening. But they're also immature, more like fetal cardiomyocytes than the cells in an adult heart.
What conditions heart-like tissue actually needs to grow

Getting stem cells to become cardiomyocytes is one challenge. Getting those cells to organize into functional tissue is a much harder one. Four factors dominate this process.
Biochemical signals
Beyond the initial differentiation, cells need ongoing growth factors to stay healthy and mature. VEGF-A encourages vascular cell development. Retinoic acid helps pattern different heart regions. Insulin, in controlled amounts, supports cell survival. Getting the timing and concentration of these signals right is more like conducting an orchestra than following a recipe.
Scaffolds and physical structure

Heart cells don't grow in a soup. In the body they're embedded in an extracellular matrix that has specific stiffness and architecture. In the lab, researchers provide either natural materials like fibrin or collagen, or synthetic hydrogels, as a 3D scaffold. The scaffold's stiffness matters: a substrate that's too soft or too rigid prevents proper sarcomere organization (sarcomeres are the little contractile units inside each heart cell). Engineered substrates can also be patterned with microgrooves or aligned fibers to guide the direction of cell growth, which is critical because heart muscle needs to pull in a coordinated direction.
Mechanical and electrical stimulation
The heart is a mechanical organ. It experiences stretch with every beat. Researchers have shown that applying cyclic mechanical stretch to engineered constructs improves cardiomyocyte alignment, sarcomere organization, and contractile force. Electrical stimulation mimics the natural pacemaker signal and drives synchronized beating, which further matures the cells. Some groups have built tissue engineering chambers that deliver continuous pulsatile electrical stimulation in vivo, allowing iPSC-derived cardiomyocytes to survive for weeks, form compact tissue, and attract host blood vessels.
Oxygen and nutrient delivery
This is the wall that organoids keep hitting. Oxygen diffuses roughly 100 to 200 micrometers into tissue before it's used up. Anything larger than that starts dying at the core unless it has blood vessels running through it. The adult heart is intensely vascularized for exactly this reason. In the lab, researchers tackle this with organ-on-a-chip systems that pump media through microchannels, co-culturing organoids with endothelial cells to encourage vessel formation, and 3D bioprinting vascular networks into constructs before seeding them with cardiomyocytes. Progress is real but scaling up remains the bottleneck.
Why building a whole heart is still out of reach
Even if you solve every tissue-level challenge above, building a whole transplantable heart involves additional problems that are genuinely unsolved right now. It helps to think of them as four distinct walls.
| Challenge | Why it's hard | Where research stands |
|---|---|---|
| Patterning | A heart has four chambers, valves, conduction nodes, and distinct muscle regions. Each region requires different cell types specified at precisely the right time and place during development. | Organoids can partially reproduce early patterning events but not full regional identity at organ scale. |
| Vascularization | A transplantable heart needs a complete coronary vasculature supplying every cubic millimeter. No engineered construct has achieved this yet. | Co-culture and bioprinting approaches work at small scale; larger constructs still face core necrosis. |
| Maturation | hPSC-derived cardiomyocytes remain fetal-like: smaller, less forceful, with different electrical properties than adult cells. This affects how safely and powerfully they'd function in a body. | Mechanical and electrical stimulation, metabolic manipulation, and prolonged culture all help but don't fully close the gap. |
| Functional integration | A transplanted heart must connect to the host's nerves, blood vessels, and conduction system without triggering fatal arrhythmias. | Heart patches have shown some integration in animal models, but whole-organ integration is entirely untested. |
Vascularization is arguably the hardest wall. You can't just build a lump of heart muscle and expect it to survive once implanted. The coronary arteries in a real heart are an intricate tree that took months to grow during development. Reproducing that from scratch, in a dish, is a problem that overlaps heavily with what researchers face when growing other complex organs like kidneys and livers from stem cells.
The hurdles described for growing other complex organs like kidneys and livers from stem cells are similar to what you would face if you asked, can you grow a kidney from stem cells? For a similar challenge of building blood supply and functional scale, the work on kidneys and livers from stem cells runs into overlap with the same vascularization wall.
How researchers actually grow and test heart tissue
Here's a high-level look at how a typical engineered heart tissue experiment runs in a research lab. This isn't a home protocol (more on that shortly) but understanding the workflow gives you a real sense of what's involved.
- Source selection: Researchers start with either commercial hPSC lines or iPSCs reprogrammed from patient cells (skin fibroblasts or blood). The cell line's genetic background affects how well differentiation works.
- Quality control: Cells are checked for pluripotency markers (OCT4, SOX2, NANOG) and genomic integrity before differentiation begins. Bad starting material means bad cardiomyocytes.
- Cardiac differentiation: The Wnt-on/Wnt-off protocol is applied over roughly 10 to 15 days in monolayer culture or as 3D aggregates, with timed additions of CHIR99021, BMP4, Activin A, bFGF, and Wnt inhibitors.
- Purification: Because not all cells become cardiomyocytes, researchers often use metabolic selection (switching to a lactate-based medium that starves non-heart cells but not cardiomyocytes) or fluorescent sorting to enrich the population.
- 3D construction: Purified cardiomyocytes are mixed with scaffold material (fibrin gel is common), cast into molds, and allowed to compact into a tissue strip or patch over one to two weeks. For organoids, aggregates are allowed to self-assemble.
- Stimulation and maturation: Constructs are placed under cyclic stretch or electrical stimulation regimes for several weeks to encourage maturation.
- Assessment: Researchers confirm success using cardiac troponin T and I staining (structural markers), calcium imaging (to visualize electrical wave propagation), force measurement (how hard the tissue contracts), and electrophysiology (action potential shape and duration).
A successful engineered heart tissue beats spontaneously, contracts with measurable force, responds to drugs like noradrenaline the way a real heart does, and shows organized sarcomere structure under a microscope. These readouts are real and reproducible. Scalable production of homogeneous cardiac organoids from hPSCs has been demonstrated, which matters for moving from one-off experiments to reliable research tools.
Where things actually stand today and what the timeline looks like
As of 2026, the most advanced clinical application is engineered heart muscle patches and cell injections for heart failure, not whole-organ replacement. Two trials are worth knowing about.
The LAPiS trial (initiated by a Keio University group) involves injecting iPSC-derived cardiomyocyte spheroids into patients with heart failure. Early reports show safety monitoring approval from independent committees, and follow-up data suggest improvements in left ventricular ejection fraction (LVEF) and functional class in some patients. A 2025 review in npj Biomedical Innovations summarizes reported clinical recruitment and early trial reports, including improvements such as LVEF and functional class and notes graft detection in follow-up improvements in left ventricular ejection fraction (LVEF) and functional class. Importantly, strategies to suppress post-transplantation arrhythmia, one of the major safety concerns, have shown promise in preclinical work.
The BioVAT-HF trial (NCT04396899) is testing epicardially implanted engineered heart muscle allografts (strips of iPSC-derived myocardium) in patients with advanced heart failure. The concept is 'biological ventricular assist tissue': not replacing the heart, but bolstering its remaining muscle. First-in-human safety data from earlier iPSC-CM patch cases showed no transplanted-cell-related adverse events over a one-year observation period.
For a realistic timeline: heart patches and cell therapies improving after heart attacks and heart failure are likely to see broader clinical use within 5 to 15 years, assuming trial results hold. A bioengineered whole heart suitable for transplantation, if it ever becomes possible, is almost certainly decades away, and many researchers think it may require growing organs inside animal hosts (xenobiotic approaches) rather than purely in vitro engineering.
Safety, ethics, and how to think about claims you'll see online
This area is full of hype and, in some cases, genuinely dangerous misinformation. Here's how to evaluate what you read.
The FDA position on stem cell therapies
In the United States, the FDA has approved exactly one category of stem cell products for general use: hematopoietic (blood-forming) stem cells from cord blood, used for blood disorders. Everything else, including heart cell therapies, is either in a clinical trial (with rigorous oversight) or unapproved. Any clinic offering a 'stem cell heart treatment' outside a registered clinical trial is operating outside FDA approval. The FDA explicitly warns that regenerative medicine products can pose serious risks, including cells migrating to unintended locations in the body and, in the worst case, forming tumors.
Tumorigenicity: the real risk with pluripotent cells
Undifferentiated pluripotent stem cells can form teratomas (a type of benign but problematic tumor) when transplanted. This is why researchers go to great lengths to purify cardiomyocytes before implantation and why regulatory agencies like the FDA, and international bodies like the ISSCR, require differentiation-status profiling and in vivo survival studies as part of any safety package. The 2025 FDA guidance on preclinical assessment of cellular therapies specifically calls out tumorigenicity risk and the need for robust endpoints.
Ethical considerations
iPSC-based heart research largely sidesteps the embryo-use debates that surrounded early ESC research, since iPSCs come from adult tissues. However, ethics questions remain around consent for donor cells, equitable access to eventual therapies, and the governance of experiments that create increasingly human-like tissue. The ISSCR 2021 guidelines provide the most current international framework for thinking through these questions, and they're worth reading if you're a student heading into this field.
How to evaluate claims responsibly
When you see a headline saying 'Scientists grow beating heart in lab,' ask these questions. Is it an organoid or a whole organ? (Almost certainly an organoid.) Was it tested in humans or animals, or just in a dish? What journal published the work, and was it peer-reviewed? Is the group that published it also selling a therapy? Peer-reviewed journals like Nature, Nature Biotechnology, and Nature Medicine are reliable; press releases from clinics selling treatments are not.
What you can actually do with this knowledge
If you're a student or educator, the most valuable next step is understanding the biology deeply rather than trying to replicate it. Cardiac organoid research requires biosafety level 2 facilities, specialized incubators, expensive reagents, and trained personnel. This is not a home science project, and attempting to culture human stem cells without proper training and regulatory compliance is both unsafe and illegal in most jurisdictions.
What you can do: explore published protocols (Nature Protocols has a detailed engineered heart tissue workflow that's freely accessible and excellent for learning). Follow the clinical trials registry at ClinicalTrials.gov to track real-world progress on cardiac cell therapies. Read the ISSCR guidelines to understand the ethical landscape. And if you're interested in the parallel challenges for other organs, the vascularization and maturation problems in heart tissue are remarkably similar to what researchers face when trying to grow liver, kidney, and pancreatic tissue from stem cells. Comparing those challenges across organ systems is one of the fastest ways to understand why whole-organ bioengineering is so difficult.
The bottom line is this: stem cell biology has given us genuinely beating heart tissue, clinically tested muscle patches, and powerful research tools. What it hasn't given us, and won't in the near future, is a lab-grown heart ready to replace a failing one.
A 2024 review categorizes in vitro cardiac development platforms such as 2D cultures, engineered substrate architectures, cardiac organoids, and embryos or explants on chip, supporting that stem-cell “heart from stem cells” capabilities are mostly at the tissue or organ-model scale rather than whole transplantable hearts a lab-grown heart ready to replace a failing one.
That honest distinction is the most important thing to carry with you. Skin cell growth from stem cells follows some of the same stem cell biology principles, but it requires different differentiation cues and culture conditions.
FAQ
When news says “scientists grew a heart,” does that mean a whole transplant-ready organ?
It is typically not a whole transplantable organ. Most “grow a heart” results are organoids or engineered tissue constructs that beat or contract for short periods in a lab setting, or patches that are tested to support damaged heart muscle, not to replace the entire heart.
Are stem-cell-derived heart cells the same as adult heart muscle?
Cardiac cells made from pluripotent stem cells usually resemble fetal-like cardiomyocytes, meaning they often show immature electrical properties and contractile behavior compared with adult heart muscle. Researchers then try to push maturation using timing-specific growth factor cues plus electrical stimulation and mechanical stretch.
Why can’t clinicians just inject stem cells, instead of purified cardiomyocytes?
If cells are transplanted before they are fully differentiated and purified, undifferentiated pluripotent cells can persist and create tumor risk. That is why safety packages generally include differentiation-status testing (for what cell types remain) and survival and tumorigenicity checks in animals before any clinical use.
What is the biggest complication after a stem-cell heart treatment, and why?
Arrhythmias are a major safety concern because immature or poorly integrated cardiac tissue can trigger abnormal rhythms after implantation. Clinical and preclinical work often focuses on strategies such as improving tissue coupling, purification, and monitoring, since electrical integration is part of both the therapeutic goal and the risk.
Can I try stem-cell heart experiments at home or in a small lab?
In most jurisdictions, attempting to culture or transplant human pluripotent stem cells outside a regulated clinical trial is unsafe and frequently illegal. Even “DIY organoid” approaches can expose you to biohazards, contamination, and severe ethical and regulatory problems, so the practical next step is learning via published methods and training in appropriate lab settings.
Why do researchers get beating cells quickly, but full tissue or implant success takes much longer?
Stem-cell-derived cardiomyocytes can beat in a dish relatively quickly, but forming a thick, long-lived tissue that survives after implantation is slower because oxygen diffusion and vascular integration are limiting. That is why the field emphasizes microchannels, endothelial co-culture, prevascularized constructs, or other strategies to speed up blood supply formation.
If the engineered tissue beats in the lab, will it automatically beat safely after transplantation?
Yes, but “wiring up” the tissue is not just about getting it to beat. Functional integration requires coordinated electrical coupling with the host myocardium, which depends on maturation, structural alignment, and connectivity, not only on cell survival.
Are stem-cell heart therapies immunologically matched to the patient?
Immunologic risk depends on the stem cell source and whether cells are patient-matched. Autologous iPSC-derived cells can reduce rejection risk, while allogeneic approaches may require additional considerations. Even with immunosuppression, electrical and vascular risks still have to be managed.
Is there one “best protocol” to make cardiomyocytes from stem cells?
Wnt-on/Wnt-off is commonly used to drive cardiac lineage commitment efficiently, but it is not the whole story. Outcome quality depends on exact timing, cell state at the start, media composition, and downstream purification, because small deviations can shift cells toward non-cardiac fates or produce more immature phenotypes.
What proof should I look for before believing a “functional heart tissue” claim?
If you are evaluating a claim, check whether the work shows organized structure and functional metrics, not just visible beating. Look for drug responsiveness, measurable contractile force, sarcomere organization, and whether experiments include relevant models for maturation and survival.
What should I do next if I want to understand the field beyond headlines?
A reliable starting point is understanding the experimental readouts researchers use to judge success, then mapping that to the bottlenecks (maturation, structure, vascularization, and electrical integration). Following clinical trial registries can also help you see which approaches are moving beyond early feasibility to safety and efficacy.
Next Article
Can You Grow a Kidney From Stem Cells Today? What’s Possible
What it means to grow kidney tissue from stem cells now, limits to whole organs, and today’s organoid progress.
