Endometriosis (almost always what people mean when they say "endo") can grow in a surprising number of places outside the uterus, but it shows up most often on the ovaries, the pelvic peritoneum, the uterosacral ligaments, and the rectovaginal septum. Less commonly, it turns up on the bladder, ureters, bowel surfaces, surgical scars, and in rare cases even the lungs or diaphragm. What determines where it can grow comes down to a very specific set of biological conditions: the tissue needs to attach, tap into a blood supply, dodge the immune system, and respond to estrogen. Without all of those things in place, a potential implant simply doesn't survive.
Where Can Endo Grow? Locations, Limits, and How to Check

Marcus Whitmore
11 May 2026

Quick note on what "endo" means here
"Endo" is used as shorthand for a lot of things in science. It shows up as a prefix in endogenous (produced from within), endocardium (inner lining of the heart), endothelium, and endometrium itself. If you landed here from a biology class question about a prefix, those are different articles. Here we're talking about endometriosis, the inflammatory, estrogen-dependent condition where endometrial-like tissue implants and grows outside the uterine cavity. That's the clinical and biological question worth unpacking.
Growth in biology: it's always about location suitability
A useful way to think about growth in any biological system is to ask: does this location give the growing thing what it needs? That applies whether you're watching a crystal form in a supersaturated solution, a root extend through soil, or a cell colony establish itself on a new surface. For living cells especially, growth isn't just about arriving somewhere. It's about surviving long enough to anchor, recruit resources, and multiply. Endometriosis is a perfect case study in how demanding that process really is.
Contrast that with non-living growth. A crystal grows wherever the chemical conditions (temperature, concentration, surface texture) are right, with no immune system to fight back and no need for oxygen. Geological formations build up over millions of years anywhere minerals can precipitate. Living tissue growth is far more conditional, which is exactly why endo doesn't just grow everywhere in the body, even though, in theory, displaced cells land in many places.
Where endometriosis actually grows in the body
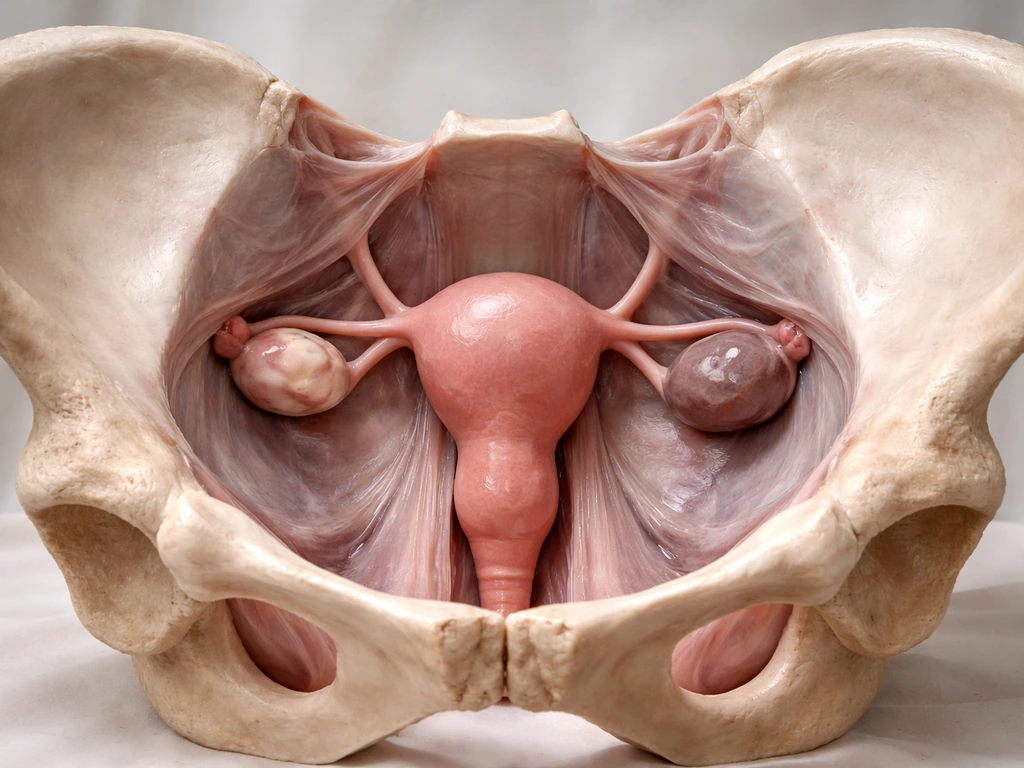
The most common picture is pelvic disease. The majority of lesions are found within the pelvis, mostly on peritoneal surfaces (the thin membrane lining the pelvic cavity) and on or inside the ovaries. When endometrioma cysts form on the ovaries, they're sometimes called "chocolate cysts" because of the old blood they contain. These are among the most recognizable lesion types.
Core pelvic sites
- Ovaries (endometriomas, or cysts filled with old blood, are a hallmark)
- Pelvic peritoneum (the lining of the pelvic cavity, where superficial lesions often appear first)
- Uterosacral ligaments (posterior compartment, often associated with deep pain)
- Rectovaginal septum (the tissue between the rectum and vagina, a site of deep infiltrating disease)
- Fallopian tubes (serosal surface or occasionally within)
- Posterior cul-de-sac (the pouch of Douglas, a common collecting point)
Less common but well-documented sites

- Bladder and ureters (urinary tract involvement, often deep infiltrating disease)
- Serosal surfaces of the bowel, including the rectum and sigmoid colon
- Abdominal and surgical scars (including caesarean section scars)
- Diaphragm (diaphragmatic endometriosis, associated with shoulder-tip pain)
- Pleural cavity and lungs (thoracic endometriosis, rare but real)
- Liver, kidneys, and gluteal muscles (extremely rare extra-pelvic reports)
There are even documented cases in people who were assigned male at birth, which tells you this condition is about cell biology and hormonal environment more than anatomy alone. That said, the vast majority of cases stay in the pelvis, and extra-pelvic disease is genuinely uncommon.
Why it can grow in those places: the biological checklist
The dominant theory for how endometriotic tissue ends up outside the uterus is retrograde menstruation. During a period, some menstrual fluid flows backward through the fallopian tubes and into the pelvic cavity instead of entirely outward. That fluid carries endometrial-like cells. Most people's immune systems clear these cells before they can establish. In endometriosis, that clearance fails, at least partly, and some cells get a foothold.
But arrival is only step one. For a lesion to actually persist and grow, a specific sequence of events has to happen. If you want the full, step-by-step view of how pulses grow, start with what conditions help endometriotic cells attach, evade immune clearance, and respond to estrogen persist and grow. Think of it like a seed that lands in soil: landing isn't enough. It needs water, nutrients, the right temperature, and no competition killing it off. For endometriotic cells, the checklist looks like this:
- Escape programmed cell death (apoptosis): the displaced cells have to survive after landing somewhere they're not supposed to be.
- Adhere to the peritoneal surface: they need to physically attach to the tissue lining.
- Degrade the extracellular matrix: essentially, they have to make room by breaking down the surrounding tissue structure.
- Generate a new blood supply (angiogenesis): lesions need oxygen and nutrients to keep growing, so they recruit new blood vessels.
- Evade immune surveillance: the local immune environment has to be permissive, or the immune system has to be somehow blunted in that area.
- Respond to estrogen: lesions are estrogen-dependent, meaning they grow and persist when estrogen levels support them, typically in the reproductive years.
The pelvic peritoneum is particularly vulnerable because it's regularly exposed to retrograde flow, it has a rich blood supply nearby, and it provides surfaces that cells can adhere to. The rectovaginal septum and uterosacral ligaments are well-vascularized, hormonally responsive areas in the deep pelvis where deep infiltrating endometriosis tends to set in. That's not coincidence. It's biology selecting for the most permissive microenvironments.
Other theories beyond retrograde menstruation include coelomic metaplasia, where cells in the peritoneal lining transform into endometrial-like cells in place, and lymphatic or vascular spread, which could explain extra-pelvic implants in distant organs. These mechanisms are less well understood but help explain why lesions occasionally appear far from the pelvis.
What stops it from growing everywhere
This is an important question, and it parallels a broader biological principle: cells that land somewhere new almost always fail. Living growth depends on the same kind of location suitability and survival factors, which also explains why do nodules grow only where the environment lets them persist. The body has layered defenses and physical constraints that limit where any tissue can establish itself.
For endometriosis specifically, the main brakes on spread are immunologic clearance (natural killer cells and macrophages in the peritoneal fluid normally destroy displaced cells), the requirement for a suitable microenvironment (not every tissue surface is chemically or structurally permissive for adhesion), vascular access (without angiogenesis, a lesion starves), and hormonal dependency (tissues that don't respond to estrogen signaling, or in postmenopausal environments with very low estrogen, are less hospitable). This is why endo is predominantly a disease of reproductive-age people and why many lesions regress after menopause.
The mechanical architecture of the body also plays a role. The pelvis is a confined, well-vascularized space with surfaces that tolerate adhesion more readily than, say, the interior of a muscle belly. Moving to more distant locations requires crossing tissue barriers and establishing vascular connections in places not optimized for it. Most displaced cells simply don't make it.
How symptoms map to locations (and why this matters)
One genuinely useful thing about endometriosis is that where it hurts often tells you (and your clinician) something about where it is. This isn't a perfect system, but symptom patterns are a real diagnostic signal. ESHRE's 2022 clinical guideline lists a constellation of symptoms to take seriously, and pairing those symptoms with anatomical knowledge helps narrow the picture.
| Symptom | Likely location to suspect |
|---|---|
| Severe period pain (dysmenorrhoea) | Peritoneal lesions, uterosacral ligaments, posterior cul-de-sac |
| Deep pain during sex (deep dyspareunia) | Uterosacral ligaments, rectovaginal septum, posterior compartment |
| Painful bowel movements or rectal bleeding cyclically (dyschezia) | Rectovaginal septum, rectosigmoid bowel surface, deep posterior disease |
| Painful urination or blood in urine cyclically (dysuria/haematuria) | Bladder or ureteral involvement |
| Shoulder-tip pain around menstruation | Diaphragmatic endometriosis, referred from diaphragmatic lesions |
| Cyclical pain near a scar (e.g., caesarean scar) | Scar endometriosis at that site |
| Chest pain or coughing blood cyclically | Thoracic/pleural endometriosis (rare, but worth flagging) |
Notice how "cyclical" keeps appearing. The estrogen-dependent, cyclically driven nature of lesion activity means symptoms that track with the menstrual cycle are a key signal, even when they seem unrelated to the pelvis at first glance. Shoulder-tip pain during a period, for instance, is easy to dismiss but can point to diaphragmatic disease.
How to actually investigate where it's growing

The honest answer here is that imaging can find a lot, but not everything. Superficial peritoneal lesions, which are often the earliest and most numerous, can be invisible on any scan. That's why a negative ultrasound or MRI doesn't rule out endometriosis. What imaging does well is map deeper disease.
Imaging options and what they're good at
Transvaginal ultrasound (TVUS) is typically the first-line imaging investigation. A skilled sonographer can identify ovarian endometriomas, assess the posterior compartment, and screen for deep infiltrating disease at sites like the rectovaginal septum, uterosacral ligaments, and bladder. The key word is "skilled" because this is operator-dependent and specialist-level ultrasound gives you far more than a standard pelvic scan.
Pelvic MRI is particularly valuable when deep infiltrating disease is suspected or when a fuller anatomical map is needed before surgery. NICE guidelines specifically recommend specialist transvaginal ultrasound or pelvic MRI for suspected deep endometriosis. ACOG’s 2026 clinical practice guideline on endometriosis diagnosis outlines recommendations for clinical evaluation, imaging, and surgical assessment to support diagnosis NICE guidelines specifically recommend specialist transvaginal ultrasound or pelvic MRI for suspected deep endometriosis.. MRI can assess the rectovaginal septum, bowel, and bladder involvement with good diagnostic performance.
For thoracic or extra-pelvic disease, CT or MRI of the chest and abdomen becomes relevant, though these are pursued only when symptoms point that way. Ultimately, the gold standard for confirming endometriosis is laparoscopy (direct surgical visualization with biopsy), which is the only way to definitively identify superficial peritoneal lesions and take tissue for histology.
What to track before your appointment
- Keep a symptom diary for at least one full menstrual cycle, noting pain location, severity (0-10), timing relative to your period, and any cyclical patterns in bowel, bladder, or other symptoms
- Note any symptoms that happen outside the pelvis but track with your cycle (shoulder pain, chest symptoms, scar swelling)
- Record the impact on daily life: missing work, needing pain medication, avoiding sex
- List any previous imaging results, surgeries, or diagnoses and bring those records
Your practical next steps today
If you're trying to figure out where your endo might be, or whether what you're experiencing is endometriosis at all, here's what to actually do:
- Start your symptom diary now, today, using the symptom-to-location table above as a guide for what to track and where pain might be pointing.
- Book an appointment with a GP or primary care provider and use the word "endometriosis" explicitly. Mention cyclical pain, any deep pain during sex, or any bowel or bladder symptoms that track with your period. Be direct.
- Ask specifically about referral to a specialist in endometriosis or a specialist gynecologist, particularly if symptoms suggest deep disease (posterior compartment pain, painful bowel movements, urinary symptoms).
- Request a specialist transvaginal ultrasound (not just a standard pelvic ultrasound) as a starting point for imaging. Ask whether your provider can refer you to a unit with experience in deep endometriosis mapping.
- If deep or complex disease is suspected based on your symptoms, ask about pelvic MRI as well. MRI gives a clearer picture of rectovaginal and bowel involvement.
- If extra-pelvic symptoms are present (shoulder-tip pain during periods, cyclical chest symptoms), flag those explicitly because they require different imaging pathways and clinicians won't always connect them without prompting.
- Understand that a normal ultrasound doesn't close the case. If symptoms are persistent and cyclical, a negative scan doesn't exclude superficial peritoneal disease. Keep advocating.
The biology of where endo can grow is genuinely interesting: it's a story about cells needing just the right environment to survive, which echoes a lot of what we see across living systems. If you are wondering what continues to grow after death, the same idea of conditions and environment applies, even though the context is very different. But the practical takeaway is that most disease stays in the pelvis, symptoms often point to location, and modern imaging combined with specialist input can map it effectively. The most important step is getting the right clinical conversation started, with your symptom pattern clearly laid out and the right questions ready.
FAQ
If my symptoms are outside the pelvis, does that mean endo is likely there too?
Not automatically. Extra-pelvic symptoms can be caused by referral pain, nerve involvement, or inflammation rather than endometriotic implants in that exact organ. A clinician usually looks for symptom timing (especially cyclical flares) and correlates it with exam and targeted imaging of likely neighboring sites first.
Can endometriosis grow in the exact same places in everyone?
No. The “typical” pattern is pelvic, but individual anatomy and how lesions evolve over time can change what develops. One person may have deep infiltrating disease in the rectovaginal septum and uterosacral ligaments, while another has more superficial peritoneal disease, which affects both symptoms and what scans can see.
If my ultrasound and MRI are normal, can endo still be present?
Yes. Superficial peritoneal lesions are often too small or subtle to detect, so a negative scan does not rule out endometriosis. If symptoms are strongly cyclical or consistent with endo, the next step is usually specialist assessment and, in some cases, laparoscopy with biopsy for definitive diagnosis.
What imaging should I ask for if I suspect deep endometriosis?
Often the most useful first step is specialist transvaginal ultrasound or pelvic MRI, because those can assess deep pelvic structures like the rectovaginal septum and uterosacral ligaments. The best choice depends on your symptoms and clinician preference, but you can request that deep disease be specifically evaluated, not just a routine pelvic scan.
Could my endo symptoms be from something else that mimics its “location” signals?
Yes. Conditions like adenomyosis, pelvic inflammatory disease, fibroids, ovarian cysts, irritable bowel syndrome, and bladder pain syndromes can overlap with endometriosis symptoms. This is why documenting how symptoms track with your menstrual cycle and which bodily triggers are involved matters when narrowing the differential.
Does endometriosis only occur in people who have periods?
No. Endometriosis has been documented in people assigned male at birth, which suggests the process is not only about menstrual anatomy. Hormonal environment and biology still matter, so clinicians may evaluate endocrine factors and consider atypical presentations when symptoms are suggestive.
How does menopause affect where endo can grow?
Endometriosis usually needs estrogen signaling to stay active, so activity often slows after menopause or with very low-estrogen states. However, “less hospitable” does not mean “impossible,” especially if you are using estrogen-containing therapy or have an alternative hormonal pattern, so ongoing symptoms should still be assessed.
If my pain is cyclical but not in my pelvis, what location should I mention to my clinician?
Bring up any cyclical pain you notice, even if it feels unrelated, and describe the pattern precisely (timing with your period, severity, and what movement or bowel or bladder activity does). For example, cyclical shoulder-tip pain is often discussed as a potential clue for diaphragmatic or thoracic involvement, which may change what workup is pursued.
What’s the difference between “endo where it can grow” and “where it does grow,” for planning next steps?
Theoretically, endometriotic tissue can implant in many locations, but most implants fail due to immune clearance, lack of a supportive microenvironment, and insufficient blood supply. Clinically, the focus is on where disease is most likely to establish given your symptoms, then using targeted imaging to confirm or rule out specific anatomical sites.
Should I track anything specific to help determine where endo might be?
Yes. Keep a simple cycle-based log noting pain locations, bowel or bladder symptoms, and whether symptoms flare before, during, or after bleeding. This helps correlate symptoms with likely sites and guides whether pelvic imaging, GI or urologic evaluation, or thoracic assessment is more appropriate.
Next Article
How Do Pulses Grow: Step-by-Step Guide to Beans, Peas, Lentils
Step-by-step guide to how pulses grow from seed to harvest, with soil, water, temps, and fixes for common failures.
